
Bargehr Group

Dr Johannes Bargehr
Immunomodulation in cardiac repair
Email: jb832@cam.ac.uk
Research
Plain English: An average heart attack wipes out around 1 billion heart muscle cells, which results in an inability of the heart to pump blood around the body (heart failure). Today there is no effective therapy available to the large number of patients in need of treatment for the loss of heart muscle. Human stem cell-derived heart muscle cells are a promising therapy, but they cannot efficiently replenish the lost heart muscle and they will require patients to take immunosuppressants to avoid a rejection. To overcome these issues the Bargehr Group modifies cell lines to make them invisible for the immune system and generate small particles that contain drugs to help heart muscle cells to survive better. They also engineer heart muscle containing immune cells that allows them to model inflammation of the heart in a dish and find new therapies.
Research Focus:
The challenge of cardiac repair
Up to 75% of patients do not survive the first 5 years after they have been diagnosed with heart failure. To date there is no scalable clinical therapy that addresses the underlying problem, which is a loss in the contractile working myocardium. It has been shown that hPSC-derived cardiomyocytes can remuscularise infarcted hearts and improve cardiac function in rodents and non-human primates. However, this is a very ineffective process with low cell retention rates and poor engraftment. Furthermore, because hPSC represent an allogeneic cell source, transplantation of hPSC-derived cardiomyocytes will require systemic immunosuppression of patients, which comes with perils on its own, such as renal failure, infection, de novo cardiovascular disease and cancer.
The Bargehr Group uses different immunomodulatory strategies to achieve better grafting efficiency of cardiomyocyte-based cell therapy, including the use of broadly immune-evasive hPSC lines that bypass cytotoxic T-cell, NK-cell, antibody-mediated and phagocytic responses, avoiding the need for systemic immunosuppression. Additionally, we are also testing the application of locally drug-eluting microparticles to avoid systemic administration of immunosuppressants. As myocardial infarction generates a hostile environment for cardiomyocyte engraftment, one line of work assesses how the recruitment of regulatory T-cells can result in a favourable modification of the myocardial niche that will allow for greater cardiomyocyte survival.
Disease modelling and drug discovery
The Bargehr Group models cardiac conditions commonly encountered in clinical practice, including myocarditis, using 3D-model systems comprised of hPSC-derived cardiomyocytes and diverse immune cell subsets. They use this disease model to elucidate the underlying mechanism of the disease process resulting in cardiomyocyte death and test if heart muscle can be rescued using different therapeutic compounds. They are also working on a scalable tissue discovery platform that is capable of medium to high throughput compound screening.
Research goals
Their work will inform on key aspects required for successful clinical translation of cardiac repair, including the need for immunosuppression and how to make cardiac cell therapy more efficacious. Cardio-immune models of myocarditis promise to provide mechanistic insights and open up new opportunities for therapeutic intervention.
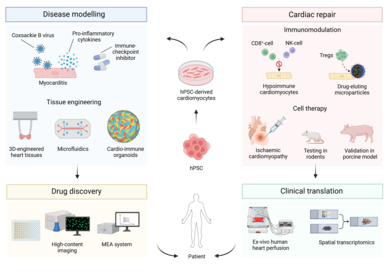
Image: Schematic of research in the Bargehr lab.

Image: Infarcted rats transplanted with hPSC-derived cardiomyocytes. Human grafts depicted in green